
Click to open a PDF version with a full table of contents
The Closure of England’s Youth Gender Identity Development Service (GIDS)
How the debate on puberty blockers plays out in New Zealand.
The Closure of England’s Youth Gender Identity Development Service (GIDS)
On 28 July 2022 the National Health Service announced the impending closure of the only child and youth gender clinic, the Gender Identity Development Service (GIDS), part of the Tavistock Hospital Trust. Its replacement will be with new services which ‘the NHS says will offer a more “holistic” approach with “strong links to mental health services”’. (Hayward et al., 2022)Moreover,
Children and young people with gender incongruence or dysphoria must receive the same standards of clinical care, assessment and treatment as every other child or young person accessing health services.(Cass, 2022)
The announcement came about after a report from the independent review by paediatrician Dr Hilary Cass (the Cass Review) which had identified serious concerns about the service (Bayswater Support, 2022) and shortly after the announcement, former equalities Minister Kemi Badenoch wrote a devastating critique of ideological capture of the UK civil servants she worked with. She was told the clinic was working well and that there was “nothing to see”.(Badenoch, 2022) The announcement was unexpected, as there were several large scale research projects still underway.
Amongst the reasons for the announcement was an assessment that the service was not safe for patients and that many practitioners had adopted ‘affirmative’ approaches to treating patients’ self-assessed gender identity, which acted to ‘overshadow’ other potential causes of their gender distress. (See Figure 1) Claiming a gender identity that differs from one’s sex can best be described as a culturally based phenomenon. The ’affirmative’ care approaches used to work with patients differ markedly from evidence-based medicine and usual scientific practice. That a gender identity is a ubiquitous part of all people is an unprovable belief. The idea that to have one that differs from one’s sex and is moreover both a normal human variation and a situation that needs urgent, and often lifelong medical intervention is unique in medicine. (SEGM, 2022) [1]
Other factors were the experimental and untested nature of the treatment; that amongst the many side effects of puberty blockers are evidence of seriously low levels of bone density (Bannerman, 2019b)(Bannerman, 2021) and the likely, but unquantified, impacts on mental development caused by puberty suppression. (Hayes, 2017) [2] The drugs are used off-label in children are the same drugs that are used to suppress the development of sex hormones in precocious puberty, endometriosis and late stage prostate cancer. Recent research has compiled the adverse effects of these drugs which are called GnHRa (Gonadotropin-Releasing Hormone Analogs) but they had not been analysed in the small cohorts treated for gender dysphoria.(Lesbians United, 2022) Another factor was that the clinic had not tracked patient outcomes for the initial experimental off-label treatment but had simply embedded it as practice. Historically research has shown that most children with gender questioning resolved this at puberty. The Cass review followed a judicial review of the clinic by a young detransitioner, Keira Bell, (High Court of Justice, 2020) and the results of an independent review of the medicine. (Cohen & Barnes, 2021) These adverse reports have allowed legal negligence cases to be mounted and cases are already in train for adult services.(Newshub, 2022) (Lane, 2022)
Worldwide there is growing concern about:
- the rapid rise in the number of children being referred for puberty blocker medication,[3]
- the unexplained change in the demographic of those presenting (from pre-pubescent to at puberty, and from mainly male to overwhelmingly female) and
- whether children can provide informed consent when the likely outcomes include sterility and anorgasmia.(Levine et al., 2022)
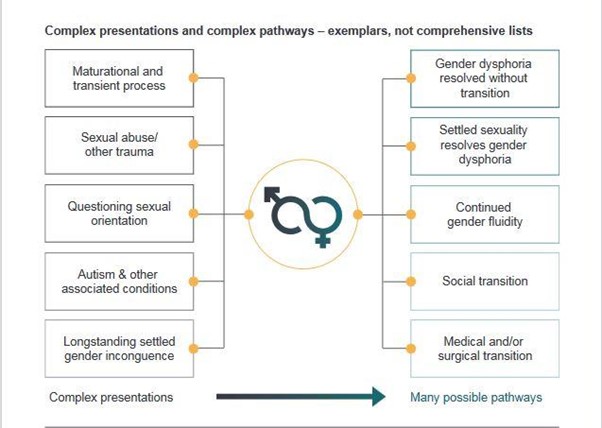
Figure 1 Image from the Cass report interim report shows gender questioning is associated with complex causation
As a result, several national level, independent, evidence-based reviews have taken place. Typical findings are that the evidence for puberty blockers is very low and there are serious known and emerging side-effects of their use. Treatment policy reversals have followed in Finland, Sweden and now in England.(Fully Informed, 2022) Several senior clinicians associated with the World Professional Association for Transgender Health (WPATH), including the President-elect, have become whistle blowers against the policies of their own organisation, calling the current affirmative model ‘sloppy care’.(Shrier, 2021)
Background resources related to the closure of GIDS
Fall of the Tavistock by Bernard Lane, a Sydney-based journalist
Clinical Damage. Times Editorial reprinted on the website of the Society for Evidence Based Gender Medicine
The Tavistock scandal shows the dangers of civil service groupthink Kemi Badenoch (Former UK Equalities minister)
Fully Informed: International institutions that have moved away from ‘affirmation only’ practices
Transgender Trend. The Tavistock gender clinic to be closed down: our response.
Transgender Trend. Why do teenage girls not want to become women?
Time for honest reflection, not defence Psychologists’ open letter to their society at their defensive response to the closure of the GIDS clinic.
How the debate on puberty blockers plays out in New Zealand.
New Zealand’s Ministry of Health retains advice that puberty blockers are safe and reversible. It says a guideline from 2018 (Oliphant et al., 2018) and WPATH advice guide treatment. In August 2021, The Royal Australasian and NZ College of Psychiatrists changed their position to argue for an exploratory differential diagnostic approach that takes account of other factors that are present with gender confused individuals.(RANZCP, 2021)
In contrast, in November 2021 the Australian and New Zealand professional associations for transgender healthcare wrote a private letter to the RANZCP (AusPATH et al., 2021) and later “decided that this letter be published in order to support broader advocacy efforts”. The research article making their case against RANZCP contains no information about the impacts or importance of major national level reviews of gender medicine.(Zwickl et al., 2022) To make its case PATHA uses some of the research articles that the national reviews found largely unconvincing and does not cite any of the national reviews explaining why it does not find them valid.
Relevance to New Zealand
The NZ Ministry of Health says that blocker medication is safe and fully reversible
The NZ Ministry of Health website claims that the medicine allows a child to avoid ‘an unwanted puberty’ (as if human maturation were a matter for choice by a child who is not considered legally competent to drive, to buy alcohol or to have a tattoo for at least another half a decade). (Ministry of Health, 2020) The Ministry is investing in greater capacity and more devolution by providing new guidelines and workforce training to meet the growing need for care. Unlike in the England, this is happening without addressing whether more of the same treatment is the best approach.(Ministry of Health NZ, 2022) The numbers are unknown because New Zealand does not collect data on prescriptions for blockers, but the ‘affirmative’ treatment is fully embedded in the 2018 NZ guideline and practice is more radical and less controlled than has happened in the England.[4] But the basic approach in using untested, off-label medicines whose data sheets expressly prohibit their use in children is the same as in the GIDS clinic had been until July. .(Teva, 2020)
Puberty blocker usage appears high in NZ and the service is highly devolved
There are few pointers to show the level of use as no data is collected, but in a Christchurch Youth clinic 65 of 100 (or 65%) of patients were on puberty blockers from a catchment population of about 600,000 (Broughton, 2021) and in 2021 a clinician from a DHB in Auckland reported 300 current patients.(Sunday Programme, 2021) Data for older patients provide some additional clues. About 30 young women at any time are seeking to raise funds for mastectomies(Give a Little, 2022) Research at the Capital and Coast District Health Board (CCDHB (covering the Wellington region of New Zealand) showed massively increasing numbers of young adults seeking cross sex hormones. That research noted there was no identifiable cause but the data does demonstrate the same increase in females and younger people noted overseas(Delahunt et al., 2018)
By contrast with the Christchurch clinic, in 2019 the Tavistock’s GIDS clinic put only 161 children onto puberty blockers in a year when there were 2519 new referrals from a population of more than 56 million. If the figures from Christchurch are typical for New Zealand the referral to medication rate is ten times higher in New Zealand than in England. (High Court of Justice, 2020) (Broughton, 2021) and the overall rate per head of population shows them to be show that the drug could be being prescribed more than 30 times more frequently per head of population in New Zealand.(Fully Informed, 2021) Gender health specialists argue in favour of their very free use in New Zealand.(Oliphant, 2017)
Compared with England, New Zealand treatment is highly devolved, with puberty blockers available from paediatric services, youth health services, endocrinologists and primary health care teams. (Ministry of Health, 2020) Standards of care are variable.(PATHA, 2021)
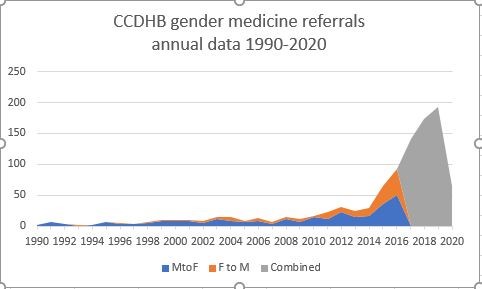
Figure 2 Data sourced from Delahunt, 2018. NB Sex data was not collected in 2018-2020. NZ was in Covid lockdown in early 2020.
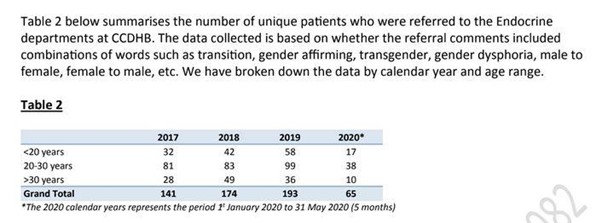
Figure 3 Screenshot from Delahunt shows rapid increase of prescribing cross sex hormones.
GIDS style ‘affirmative only’ treatment is embedded in NZ policy and law
Even as the Cass report and the other reviews are showing that other issues are in play, NZ‘s professional bodies and guidelines argue for affirmative only care.[5] The approach avoids diagnosis in favour of a belief that children and young people are transgender if they say so (Psychologists Board, 2019) and they are each on ‘a unique journey to affirm….gender’ (Oliphant, 2018)(Psychologists Board, 2019) and they are each on ‘a unique journey to affirm….gender’ The parliamentary debates on the 2022 Conversion Practices Prohibition Legislation also were also in favour of affirmation and the wording of the new law reflects this.(Parkinson & Morris, 2021) This especially impacts counsellors who, because they are not ‘registered health practitioners’ have no specific protections for working within their scope of practice.(NZ Government, 2022) The New Zealand Association of Counsellors (NZAC), had apparently not advocated with government to preserve their standing as professionals with an exploratory role. Instead, NZAC relies on a code of practice that is ‘affirmative only’ towards people who have gender dysphoria. Thus their practice model explicitly prevents the investigation of overshadowing issues as is the case for NZ psychologists.
The CATA conference: Children, Adolescents and Gender
In May 2022, the Child and Adolescent Counselling Association (CATA), a small group of counsellors and psychotherapists who run an annual professional development event, announced the topic of their forthcoming conference. CATA is aware of the developing situation overseas and the issues with affirmative care. CATA members are concerned that clients are being channelled towards puberty blockers – and their conference Children, Adolescents and Gender: Impacts of transgender ideology included clinicians, parents, lesbians, teachers and young people who have detransitioned. At the conference they provided evidence of the harms of affirmative treatment. Lawyers explained how counsellors and others might work within the new law on conversion practices prohibition. Commentary from Australia notes that where similar legislation exists, some counsellors will avoid working with children on gender and sexuality issues altogether because they see exploratory counselling as having been criminalised.(Parkinson & Morris, 2021)
Bullying and intimidation: The battle of ideas about gender questioning
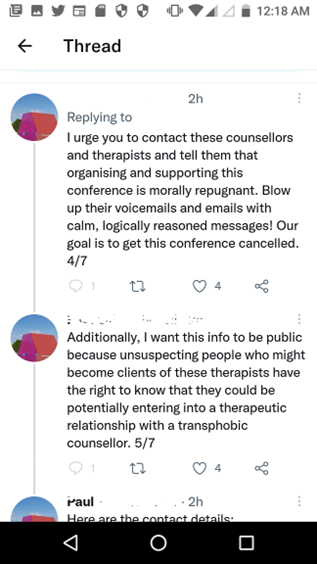
After announcing the conference, the CATA organisers had their contact details released online by activists who encouraged others to call them repeatedly and to threaten their employment. Their own professional association, the New Zealand Association of Counsellors, denounced the conference without apparently having spoken to the organisers. Activists petitioned the proposed venue and made calls threatening to boycott it indefinitely if it hosted the conference(Teens Against TERFS, 2022)Speakers were targeted to the point where one withdrew.(Rivers, 2022) In the light of these threats, the final venue was not announced until the day prior to the event itself and the conference was held mostly online.
After it was announced in May the conference was effectively denounced by news website Stuff NZ in an entirely one-sided article (Hubbard, 2022) as well as by the NZ Psychological Society.(NZPS, 2022) NZAC and NZPS claimed that the conference approach did not reflect evidence-based best practice in working with transgender or gender-diverse children and adolescents. Nonetheless the organisers defended their right to proceed (Stuff NZ staff reporter, 2022)
Like NZAC the NZPS takes its lead from US-based organisations like the World Professional Association for Transgender Health (WPATH), the American Association of Paediatricians (AAP) and the American Psychological Association (APA), whose guidelines also endorse only affirmative medicine. But those ‘affirmative’ guidelines are sourced from an ideological set of assumptions that support self-diagnosis for even very young children and the detailed reviews discussed above are ignored. (Irvine, 2022) (Bayswater Support, 2022)[6]
There is a stark contrast between gender ideology approaches that contain the idea that we each have a gender identity that must be matched by medication and surgery to align with the patient’s wishes and the evidence-based reviews that are identifying serious harms.
Discussion
The most robust evidence about puberty blockers, and also the most recent, is contained in the independent reviews of gender medicine that have come out against rushing to medicine to suppress puberty in favour of exploration and a cautious approach. The GIDs approach was an experiment that was never completed or reported on and where the publishing that did occur was incomplete and ridden with omissions and errors. Nonetheless it was reported in the media as a success and was embedded as standard practice. However in contrast to the RANZCP and CATA, neither the Ministry of Health, New Zealand health and mental health practitioners, nor PATHA have responded to these important developments overseas.
Child and youth gender medicine in New Zealand involves the same experimental treatments that were being used at GIDS but they are still regarded as being safe and reversible. The serious harms that are caused by puberty blockers, and the overdiagnosis have not yet raised alarm bells. Adult transgender people have participated in the bedding in of affirmative policies for gender questioning children and youths, even though most children would have desisted without treatment. The available data shows that children may be being medicated in New Zealand, more readily than in England, both as a proportion of referrals and as a proportion of population. The affirmative approach taken in NZ law, policy and professional guidelines means that overshadowing effects can neither be identified, nor overcome without the professionals involved potentially risking professional or legal censure.
How is it possible that in one country a clinic is closed as unsafe but where a laxer and more permissive regime is in place there are no concerns? Or does the careless approach noted by the WPATH whistle-blowers represent what is happening in New Zealand? Perhaps it is also the case that our Associate Minister of Health is being told that our youth gender medicine regime is working well and that there is nothing to see.
The rest of this article is a series of appendices providing background on the issues outlined above.
Author Biography
I am an independent researcher working on issues of sex and gender. I am a former public servant as a policy advisor on topics related to information and the internet as well as an information manager and librarian. My twin reasons for involvement in this topic are a desire to see good evidence-based public policy enacted. As a lesbian my involvement is personal. It is heart-breaking to see the new generation of would-be lesbians (as well as many other young men and women) deciding that their lives are better lived in hiding from themselves.
This research has not been peer-reviewed, and is my own independent work so although I have referenced each claim any errors are my responsibility.
Co-author of Sex, gender and women’s rights (Rivers & Abigail, 2021)and Another Unfortunate Experiment (Rivers & Abigail, 2020)
Appendix 1: Background to the Tavistock GIDS clinic closure
The Cass review followed: a 40-fold increase in numbers; long waiting lists, an unexplained change [7] from the usual cohort of very young boys to a novel cohort of girls and young women at and beyond puberty; a large number of resignations (Donnelly, 2019); whistle-blower allegations (Entwistle, 2019); and “dark stories by practitioners that if current practice continued there would be no homosexuals left” (Bannerman, 2019a)
The GIDS experiment on the impact of puberty blockers in treatment was begun in 2011, but rather than reporting on its impacts the data was never analysed. It was reported in the press as a success and the treatment path was embedded as practice.(Biggs, 2020) NHS advice that they were considered to be fully reversible was replaced in June 2020 with a statement that “little is known about the long-term side effects of hormone or puberty blockers in children with gender dysphoria,”(Kirkup, 2020) and a judicial review where a young woman, Keira Bell, argued she had been medicated and operated on without an adequate diagnosis (Holt, 2020) have also been significant. Research presented at the Keira Bell trial[8] was carried out by New Zealander Michael Biggs, an Associate Professor with the Department of Sociology at Oxford University. It provided much of the evidence that supported the whistle blower testimony and drew public attention to the deficiencies which led ultimately to the closure announcement(Biggs, 2020) This evidence is summarised below.
Appendix 2: Gathering the evidence of harm – the Biggs dossier
Dr Biggs’ published five separate research articles using the published data from GIDS research, annual reports and other published material, and re-analysed it together with data gained from FOIA enquiries. He found that:
Between 2010 and 2014, puberty blockers were given to 44 children. This study yielded only one published scientific article on outcomes. In addition, there is unpublished evidence. Yet the study has been used to justify rolling out this drug regime to several hundred children aged under 16. Almost five years after the last patient was enrolled in the experiment, there is no evidence to substantiate Carmichael’s claim that “the results thus far have been positive”.[9]
Dr Biggs found that:
- The treatment was experimental and the medication Gonadotropin-Releasing Hormone agonists (GnRHa) (known in their usage in gender questioning children as puberty blockers) have not been certified for use and are not certified as safe or effective.
- Research on the use of puberty blockers was scoped in 2010, but after 2015 the Research Ethics Committee forgot that the treatment was an experiment, as did the head of the GIDS clinic.
- Puberty blockers were routinely being given to children from the age of 12, and in some cases as young as 10.
- Using the information available from diverse sources it was found that:
- Children were missing from the research data, sets with no explanation and conference papers showing negative results for girls were never published
- The reports that were produced included misleading references, for example a information was provided that bone density did not decrease over the course of treatment when adolescence is the time when bone density increases rapidly. A low rise in bone density is a potential indicator of early onset osteoporosis
- After a year on GnRHa, children reported greater self-harm. Girls experienced more behavioural and emotional problems and expressed greater dissatisfaction with their body, showing that puberty blockers exacerbated their gender dysphoria compared to boys.
- There was no evidence for the effectiveness of GnRHa;
In the only published paper from the study all the negative results were initially omitted. The abstract said that children with puberty blockers had statistically significant improvement in psychosocial functioning over a group given only psychological support. But the data found that the two groups were similar.(Costa et al., 2015) Furthermore:
- Clinicians reported that they had succumbed to pressure from families and transgendering organizations like Mermaids, which lobbied vigorously to lower the age at which GnRHa drugs were administered to children
- Information that boys who took GnRH from early puberty would still have the penis and testes of a pre-pubescent boy and thus would have insufficient tissue to create a neo-vagina (necessitating the use of grafted rectal tissue for this purpose) was known but was not on the Parent Information Sheet they gave to children and carers.
- The missing research requested for the court case was only published to a pre-publication server the day after the trial result was announced.(Carmichael et al., 2020) It showed that all but one of the participants continued to cross-sex hormones. This, together with other earlier reports on levels of continuation to cross sex hormones, belies the idea that puberty blockers provide ‘a pause to decide’(Biggs, 2020)
Further, Dr Biggs reports that the original research project scoped in 2010 said that
assessment of growth, bone health and psychological outcomes will be important to assess the medium and long-term safety and effectiveness of early intervention.
- However, Dr Biggs reports that the resulting research was compromised in any case because:
GIDS apparently failed to collect any data on its experimental subjects after they turned 18. In a startling admission, Carmichael and co-authors blame ‘the frequent change in nominal and legal identity, including NHS number in those referred on to adult services’—‘to date they have not been able to be followed up’.
Appendix 3: The Keira Bell court case
The Keira Bell court case, R (on the application of) Quincy Bell and A -v- Tavistock and Portman NHS Trust and others was partially overturned on appeal. This ensured that prescribing remained a matter for doctors and not for the courts but the substantive findings remained in place. The court case reiterated Dr Biggs’ findings that
- GIDS failed to collect basic data and to report outcomes
- The treatment is experimental and has unknown long-term effects
- For nearly all children, puberty blockers continued inexorably to further treatment [meaning that they are not the “pause button” that is so often claimed].
- The permanence of changes to a young person’s life, including irreversible loss of sexual function and fertility, meant that children and young people were unable to give informed consent because they could not understand the impacts of these changes on their lives.(High Court of Justice, 2020)
The informed consent issues were laid bare in testimony.
“One of the GIDS’ witnesses, “J” embarked on puberty suppression at the age of 12. According to J’s recollection of the consent process: “We discussed sex and I told them the idea of it disgusted me. I knew I would be unable to consider having a sexual relationship as an adult with my body so wrongly formed” .(High Court of Justice, 2020, para 86)
As a result, the judges wrote
“Some of the children and young people who have been treated at GIDS say in their witness statements that the thought of sex disgusted them, or they did not really think about fertility. These normal reactions do not detract from the difficulties surrounding consent and treatment with PBs. That adolescents find it difficult to contemplate or comprehend what their life will be like as adults and that they do not always consider the longer-term consequences of their actions is perhaps a statement of the obvious.” (High Court of Justice, 2020 para 141)
Appendix 4: Comparing practice in New Zealand with GIDS
New Zealand’s practice is similar to the now abandoned approach in England, but appears to be potentially more lax and to have endorsed an ‘affirmation’ approach with greater commitment than the GIDS clinic did. The NZ guidelines advise following the lead of the patient towards their preferred gender expression (Oliphant et al., 2018) but are embedded in the guidelines rather than being the approach of some practitioners, as it was at GIDS. The medicines deployed are the same GnRHa that are experimental, untested and used off-label as those used in England, but they are used more freely with no data collection.
As in England, male puberty blocker patients are not told in the informed consent data sheets that if suppressed throughout puberty there will be insufficient tissue to create a neo-vagina. For both sexes, issues related to sterility are cast in the language of ‘fertility preservation’.
Figure 4Table of differences in gender medicine between the England and NZ
| Approach | NZ | GIDS |
| Early social transitioning | Encouraged. (which can harden a transgender identity) | Not supported |
| Data gathering | No national data is collected on numbers or outcomes of children on puberty blockers. | Data on raw numbers of referrals and patients receiving puberty blockers is collected. |
| Service delivery | Highly devolved including to youth clinics and GP practices. | Specialist hospital based service. Centralised with well controlled access |
| Diagnosis | No formal diagnosis: affirmative of the patient’s self-assessed gender. | Several sessions to explore issues. |
| Proportion of children of the relevant cohort on puberty blockers | 65%(Fully Informed, 2021) (These are indicative only, from press reports, as treatment figures are not collected in NZ) | Approximately 6% (High Court of Justice, 2020) (Children are not necessarily medicated in the same year that they are referred. The comparison is between referrals and prescriptions for 1 year.) |
| Advise effects of puberty blockers | Administered very freely to age 20 with no time limits on use. (Oliphant, 2017) “Safe and fully reversible” (Ministry of Health, 2020). Still on website 2022 | Used from early puberty to 16. The advice has changed to now say “little is known about the long-term side effects of hormone or puberty blockers in children with gender dysphoria”. (Kirkup, 2020) |
| Policy making | National decision making on whether medications are safe is devolved to gender health specialist practitioners. (OIA supplied by email). | The NHS describes the required service and it has been delivered by GIDS. The scope is not explicitly affirmative. No overall standard of delivery and practice is very mixed. |
| Activist involvement | Adult activists are fully involved with gender identity medicine policy-making including for children and young people, and were fully involved in the development of the NZ guidelines. (Oliphant et al., 2018) | The involvement of activists in determining policy was recognised as problematic.(Turner, 2020a) |
| Explanation for increase | There has always been the same number of transgender people. Lowered stigma accounts for the number seeking treatment(Sunday Programme, 28 February 2021) | No specific explanation |
| The philosophical approach to the guidelines. | The guidelines fully embed gender identity ideology, including citing the supposed gender variance of indigenous Māori. (Oliphant et al., 2018) | Gender identity ideology and affirmative approaches have been adopted by many clinicians but are not ‘baked-in’ to the NHS approach. (NHS England, 2018) |
| Puberty blockers act as a pause button | Ministry of Health advises that blockers provide time to decide whether gender change is the right decision | Information about safety and reversibility has been removed.(Kearns, 2020) |
| Mental health | Mental health problems are ascribed mostly to stigma. They are not a bar to seeking treatment. Not being able to give verbal consent is no bar to treatment. | Mental health issues if present must be reasonably well controlled. |
| Psychosocial assessment | Information that up to 75% of gender confused children do not persist with a cross gender identity was removed from the current version of the NZ guidelines.(Strongman, 2019) Neither having mental health issues nor being unable to provide informed consent is a barrier to accessing gender affirming services. Transgender people…able to able to make informed choices for themselves regarding gender affirming care. (Oliphant et al., 2018) | Most treatments offered at this stage are psychological rather than medical. This is because in many cases gender variant behaviour or feelings disappear as children reach puberty(NHS England, 2018) |
| Language | Fully adopts the language of gender ideology and affirmation. | The language used in official documents is neutral. |
| Level of reticence to speak out. | Few clinicians are yet visible with their concerns and there is little media coverage of the issues. | Dozens of clinicians have spoken of their concerns and there has been extensive media coverage of the issues. |
| Media coverage | Until a recent article in NewsRoom (Donovan, 2022) there was no coverage critical of the affirmative approach. Amongst the minimal coverage was positive reporting on published research that does not exist (University of Otago, 2021) and those with concerns have been insultingly equated with conspiracy theorists who believe that we are governed by a race of lizard people. (Media Council, 2022) | Concerns about puberty blockers have been covered in almost every major media outlet. |
Appendix 5: The origins of affirmative only treatment
New Zealand’s practice has followed the lead of overseas professional associations and WPATH and it is predicated on affirming the child or young person’s gender identity. Affirmation has been championed by Diane Ehrensaft and others whose work is referenced in the New Zealand guidelines (Oliphant et al., 2018) on the basis of a series of assumptions about the nature of gender identity (Ehrensaft, 2016) that are not based on scientific or medical evidence but in post-modern queer theory(Bayswater Support, 2022)There are claims that are not supported in either science or medicine, such as that:
- gender can be observed in very young children who pull apart clothing or remove hair ornaments to indicate their gender is different from their sex (Ehrensaft, 2018)
- everyone has a gender identity that may or may not align with their sex and which may be fluid
- gender is evidenced by personal stylistic preferences and choices and by differing from cultural norms
- psychological problems suffered by a person with a gender identity different from their sex are generally caused by stigma rather than by co-morbid associations of the cross-gender belief.
From this perspective, analysis and diagnosis are precluded because the person’s self-perception is paramount. A gender identity disparate from sex is regarded as merely a normal variation, even though it may require lifelong medication and multiple forms of surgery. (As such, gender differs starkly from other disorders of self-perception, such as anorexia and the appearance medicine demanded in response to perceptual abnormalities like elective amputations. These conditions are not endorsed as becoming one’s ‘real self’.) The primacy of reporting a gender identity that ‘needs’ medical attention also serves to overshadow other causes of gender confusion such as same-sex attraction, trauma (including the high frequency in ‘looked after children’) or autism syndrome conditions. There is also speculation that some are affected by social contagion and some girls simply see being female as a very undesirable option. See appendix 6 below.
Figure 2 Image from a presentation by Diane Ehrensaft. Principles underlying the gender affirmative model.
Appendix 6: Social contagion and why girls don’t want to be girls.
Lisa Littman coined a descriptive term Rapid Onset Gender Dysphoria(POGD) to describe the sudden increase in pubescent and post pubescent girls seeking to transition. She used parent reports of their children’s circumstances and found that there were elements of social contagion such as many girls in the same friendship group changing their gender identification at the same time. (Marchiano, 2017)
Lisa Marchiano (Marchiano, 2017) is a Jungian psychologist who speculated that the decision to transition has similarities with the social contagion that has been associated with self-harm, especially cutting and anorexia.
Transgender Trend has written speculatively about the social expectations imposed on girls and young women as reasons that they do not want to grow up to be women. (Turner, 2020b) Abigail Shrier’s book covers similar territory(Turner, 2020b)
References
AusPATH, PATHA, & et al. (2021, November). Joint Letter to RANZCP – AusPATH. https://auspath.org.au/2021/11/30/joint-letter-to-ranzcp/
Badenoch, K. (2022, July 29). The Tavistock scandal shows the dangers of civil service groupthink. https://www.thetimes.co.uk/article/the-tavistock-scandal-shows-the-dangers-of-civil-service-groupthink-5bj2z26c7
Bannerman, L. (2019a). It feels like conversion therapy for gay children, say clinicians. The Times. https://www.thetimes.co.uk/article/it-feels-like-conversion-therapy-for-gay-children-say-clinicians-pvsckdvq2
Bannerman, L. (2019b, July 26). Puberty blocking drugs: ‘For the past four years I’ve been stuck as a child’. https://www.thetimes.co.uk/article/transgender-children-puberty-blocking-drugs-for-the-past-four-years-i-ve-been-stuck-as-a-child-5s6tkh7z2
Bannerman, L. (2021, February 3). Puberty blockers ‘stunt bone growth of children’. https://www.thetimes.co.uk/article/puberty-blockers-stunt-bone-growth-of-children-tlv8qmdcd
Bayswater Support. (2022). A History of Affirmation. Bayswater Support. https://www.bayswatersupport.org.uk/a-history-of-affirmation/
Biggs, M. (2020). The Tavistock’s Experiment with Puberty Blockers. Oxford University. http://users.ox.ac.uk/~sfos0060/Biggs_ExperimentPubertyBlockers.pdf
Broughton, K. (2021, March 8). Call for more research into use of puberty blockers | Stuff.co.nz. Stuff NZ. https://www.stuff.co.nz/national/health/124409488/call-for-more-research-into-use-of-puberty-blockers
Cass, H. (2022). Interim report – Cass Review. The Cass Review. https://cass.independent-review.uk/publications/interim-report/
Cohen, D., & Barnes, H. (2021, April 9). Evidence for puberty blockers use very low, says NICE -. BBC. https://www.bbc.com/news/health-56601386
Costa, R., Dunsford, M., Skagerberg, E., Holt, V., Carmichael, P., & Colizzi, M. (2015). Psychological support, puberty suppression, and psychosocial functioning in adolescents with gender dysphoria. The Journal of Sexual Medicine, 12(11), 2206–2214. https://doi.org/10.1111/jsm.13034
Delahunt, J. W., Denison, H. J., Sim, D. A., Bullock, J. J., & Krebs, J. D. (2018). Increasing rates of people identifying as transgender presenting to Endocrine Services in the Wellington region. New Zealand Medical Journal, 131(1468), 10. https://www.nzma.org.nz/journal-articles/increasing-rates-of-people-identifying-as-transgender-presenting-to-endocrine-services-in-the-wellington-region
Donnelly, L. (2019, December 12). Children’s transgender clinic hit by 35 resignations in three years as psychologists warn of gender dysphoria ‘over-diagnoses’. The Telegraph. https://www.telegraph.co.uk/news/2019/12/12/childrens-transgender-clinic-hit-35-resignations-three-years/
Donovan, S. (2022, August 18). Parents of gender-questioning kids being let down. Newsroom. https://www.newsroom.co.nz/ideasroom/page/gender-questioning-kids-being-let-down
Ehrensaft, D. (Director). (2016, October 8). Apples, Oranges, and Fruit Salad: Sorting Out Transgender, Gender Diverse, and Beyond Gender Children and Youth. https://vimeo.com/186051984
Ehrensaft, D. (Director). (2018, July 23). How to tell if babies are transgender? https://www.youtube.com/watch?v=M7KBZeRC1RI&feature=youtu.be
Entwistle, K. (2019). An Open Letter to Dr Polly Carmichael from a Former GIDS Clinician (Medium). https://medium.com/@kirstyentwistle/an-open-letter-to-dr-polly-carmichael-from-a-former-gids-clinician-53c541276b8d
Fully Informed. (2021). Puberty Blockers—Your Obligations as GPs. Fully Informed. https://fullyinformed.nz/gp
Fully Informed. (2022). Institutional evidence based studies of puberty blockers. Fully Informed. http://localhost:3000/docs/institutions/
Give a Little. (2022). Fundraisers for ‘Top Surgery’ i.e. Elective double mastectomy. https://givealittle.co.nz/search?q=%27top+surgery%27
Hayes, P. (2017). Commentary: Cognitive, emotional, and psychosocial functioning of girls treated with pharmacological puberty blockage for idiopathic central precocious puberty. Frontiers in Psychology, 8(JAN), 1053. https://doi.org/10.3389/fpsyg.2017.00044
Hayward, E., Bannerman, L., & Ames, J. (2022, July 28). Tavistock child gender clinic forced to close over safety fears | News | The Times. The Times. https://www.thetimes.co.uk/article/tavistock-child-gender-clinic-forced-to-close-over-safety-fears-2gfj325lt
High Court of Justice. (2020). R (on the application of) Quincy Bell and A -v- Tavistock and Portman NHS Trust and others. Courts and Tribunals Judiciary. https://www.judiciary.uk/judgments/r-on-the-application-of-quincy-bell-and-a-v-tavistock-and-portman-nhs-trust-and-others/
Hubbard, C. (2022, June 10). Transgender conference sparks fierce national backlash. Stuff.Co.Nz. https://www.stuff.co.nz/national/128897870/transgender-conference-sparks-fierce-national-backlash
Irvine, L. (2022). Clinical standards and negligence in gender identity services. British Medical Journal. https://www.bmj.com/content/378/bmj.o2016/rr
Kearns, M. (2020, June 4). The NHS Quietly Changes Its Guidance for Gender Dysphoric Children. National Review. https://www.nationalreview.com/corner/the-nhs-quietly-changes-its-guidance-for-gender-dysphoric-children/
Kirkup, J. (2020). The NHS has quietly changed its trans guidance to reflect reality. The Spectator. https://www.spectator.co.uk/article/the-nhs-has-quietly-changed-its-trans-guidance-to-reflect-reality
Lane, B. (2022). Tavistock faces potential class action lawsuit [Substack newsletter]. Gender Clinic News. https://genderclinicnews.substack.com/p/tavistock-faces-potential-class-action
Lesbians United. (2022). Puberty Suppression Medicine or Malpractice.pdf. https://lesbians-united.org/organizationMaterials/Puberty%20Suppression%20Medicine%20or%20Malpractice.pdf
Levine, S. B., Abbruzzese, E., & Mason, J. W. (2022). Reconsidering Informed Consent for Trans-Identified Children, Adolescents, and Young Adults. Journal of Sex & Marital Therapy, 0(0), 1–22. https://doi.org/10.1080/0092623X.2022.2046221
Marchiano, L. (2017). Outbreak: On transgender teens and psychic epidemics. Psychological Perspectives, 60(3), 345–366. https://doi.org/10.1080/00332925.2017.1350804
Media Council. (2022). Jan Rivers against TVNZ. Media Council. https://www.mediacouncil.org.nz/rulings/jan-rivers-against-tvnz/
Ministry of Health. (2020). Transgender New Zealanders: Children and young people. Ministry of Health. https://www.health.govt.nz/your-health/healthy-living/transgender-new-zealanders/transgender-new-zealanders-children-and-young-people
Ministry of Health NZ. (2022). Budget 2022: Vote Health. https://www.health.govt.nz/about-ministry/what-we-do/budget-2022-vote-health
Newshub. (2022, June 24). UK transgender patient suing National Health Service after changing mind about reassignment surgery. Newshub. https://www.newshub.co.nz/home/world/2022/06/uk-transgender-patient-suing-national-health-service-after-changing-mind-about-reassignment-surgery.html
NHS England. (2018). Gender development service children adolescents. https://www.england.nhs.uk/wp-content/uploads/2017/04/gender-development-service-children-adolescents.pdf
NZ Government. (2022). Conversion Practices Prohibition Legislation Act 2022 No 1, Public Act – New Zealand Legislation. https://www.legislation.govt.nz/act/public/2022/0001/latest/whole.html
NZPS. (2022). Statement on CATA Conference. New Zealand Psychological Society(NZPS). https://www.psychology.org.nz/application/files/2416/5483/3126/Statement_on_CATA_Conference.pdf
Oliphant, J. (Director). (2017, November 9). PHARMAC seminar: Diversity and inclusive primary healthcare, 2a. Gender diversity, part 1. https://www.youtube.com/watch?v=NKD3gR9l_Ag
Oliphant, J., Veale, J. F., MacDonald, J., Carroll, R., Harte, M., Stephenson, C., & Bullock, J. J. (2018). Guidelines for gender affirming healthcare for gender diverse and transgender children, young people and adults in Aotearoa. Transgender Health Research Lab, University of Waikato,. https://researchcommons.waikato.ac.nz/bitstream/handle/10289/12160/Guidelines%20for%20Gender%20Affirming%20Health%20low%20res.pdf
Parkinson, P., & Morris, P. (2021). Psychiatry, psychotherapy and the criminalisation of ‘conversion therapy’ in Australia. Australasian Psychiatry, 29(4), 409–411. https://doi.org/10.1177/10398562211014220
PATHA. (2021). An update on gender affirming care provision across Aotearoa. Professional Association for Transgender Health Aotearoa. https://www.patha.nz/News/12209428
Psychologists Board. (2019). Best Practice Guideline: Working with sex, sexuality, and gender diverse clients. 22. https://psychologistsboard.org.nz/wp-content/uploads/2021/06/Sex-sexuality-and-gender-diversity-270819.pdf
RANZCP. (2021). Recognising and addressing the mental health needs of people experiencing Gender Dysphoria / Gender. Royal Australian and New Zealand College of Psychiatrists. https://www.ranzcp.org/news-policy/policy-and-advocacy/position-statements/gender-dysphoria
Rivers, J. (2022). The New Zealand Association of Counsellors capitulates to pressure from trans-activists. https://www.publicgood.org.nz/2022/06/21/the-new-zealand-association-of-counsellors-capitulates-to-pressure-from-trans-activists/The New Zealand Association of Counsellors capitulates to pressure from trans-activists
Rivers, J., & Abigail, J. (2020). Another Unfortunate Experiment? New Zealand’s transgender health policy and its impact on children. https://www.publicgood.org.nz/2020/12/02/another-unfortunate-experiment/
Rivers, J., & Abigail, J. (2021). Sex, Gender and Women’s Rights. Policy Quarterly, 17(4), 38–49. https://doi.org/10.26686/pq.v17i4.7316
SEGM. (2022, July 29). Clinical Damage: The Tavistock Clinic’s closure follows a damning report on ideological malpractice | SEGM. The Times. https://www.segm.org/Tavistock-closure-the-times
Shrier, A. (2021). Top Trans Doctors Blow the Whistle on ‘Sloppy’ Care. Common Sense with Bari Weiss. https://bariweiss.substack.com/p/top-trans-doctors-blow-the-whistle
Strongman, S. (2019, February 6). Sex self-identification debate a ‘cesspool of harmful stereotypes’. RNZ. https://www.rnz.co.nz/news/in-depth/381878/sex-self-identification-debate-a-cesspool-of-harmful-stereotypes
Stuff NZ Staff reporter. (2022, June 26). Transgender conference organisers defend right to proceed. Stuff NZ. https://www.stuff.co.nz/national/129033718/transgender-conference-organisers-defend-right-to-proceed
Sunday Programme. (2021). The controversial treatment preventing puberty for transgender kids. TVNZ. https://www.tvnz.co.nz/one-news/new-zealand/controversial-treatment-preventing-puberty-transgender-kids
Teens Against TERFS. (2022). Cancel CATA’s Transphobic Conference. Change.Org. https://www.change.org/p/cancel-cata-s-transphobic-conference
Teva. (2020). Data Sheet Goserelin (Teva). Teva. https://pharmac.govt.nz/assets/Uploads/2020-Goserelin-Brochure-for-Prostate-Cancer.pdf
Turner, J. (2020a, April 1). Giving puberty blocker to ‘trans’ children is a leap into the unknown. The Times. https://www.thetimes.co.uk/article/giving-puberty-blocker-to-trans-children-is-a-leap-into-the-unknown-x3g37sb7f
Turner, J. (2020b, December 20). Irreversible Damage by Abigail Shrier review—Resisting the ‘transgender craze’. The Times. https://www.thetimes.co.uk/article/irreversible-damage-by-abigail-shrier-review-resisting-the-transgender-craze-8mzrt3gk9
Zwickl, S., Chaplin, B., Bisshop, F., Cook, T., Soo, C. T. M., Birtles, B., Veale, J., Carroll, R., Johnson, R., Macdonald, J., Porter, J., Withey-Rila, C., Kristensen, Z., & Lin, A. (2022). Re: The RANZCP position statement on gender dysphoria. Australian & New Zealand Journal of Psychiatry, 000486742211120. https://doi.org/10.1177/00048674221112007
[1] See appendix 1 for more information on the closure of the GIDS clinic and appendix 2 for more information on the harms caused by puberty blockers.
[2] See appendices 2 and 3 for more information on the health issues with puberty blockers and the operation of the Tavistock GIDS clinic.
[3] While the change is unexplained there is plenty of theorising. Some is detailed below in appendix 6.
[4]See appendix 4, which contrasts NZ and GIDS practice with puberty blockers.
[5] See appendix 4 to compare practice in England and Wales and in NZ and appendix 5 on how affirmative care has come about.
[6] Appendix 5 has information on the origins of the affirmative approach, which is contrasted with evidence- based medicine.
[7] See appendix 6 for some theorising on the reasons why growing numbers of children have gender issues. .
[8] See appendix 3 for more information about the Keira Bell trial.
[9] Other work by Dr Biggs has found that claims of suicidality by children with gender dysphoria have been overstated and that NGO funding has been used to memorialise a supposed tsunami of murders of transgender people across the world that does not appear to be supported by the available data.

Latest Comments